
胃食管反流病(专业版)
胃灼热或烧心是胸骨后的烧灼感,它是由许多不同的原因造成的。偶然发生的烧心,一般不造成健康问题,而慢性胃灼热,每周出现几次、持续发生几周且反复发生,这就是胃食管反流病.
英文名称:Gastro-oesophageal Reflux Disease,GERD;Chronic Heartburn
定义
胃灼热或烧心是胸骨后的烧灼感,它是由许多不同的原因造成的。偶然发生的烧心,一般不造成健康问题,而慢性胃灼热,每周出现几次、持续发生几周且反复发生,这就是胃食管反流病(GERD)。胃酸反流刺激食管,随着时间的推移,可造成永久性损伤甚至癌变。病因
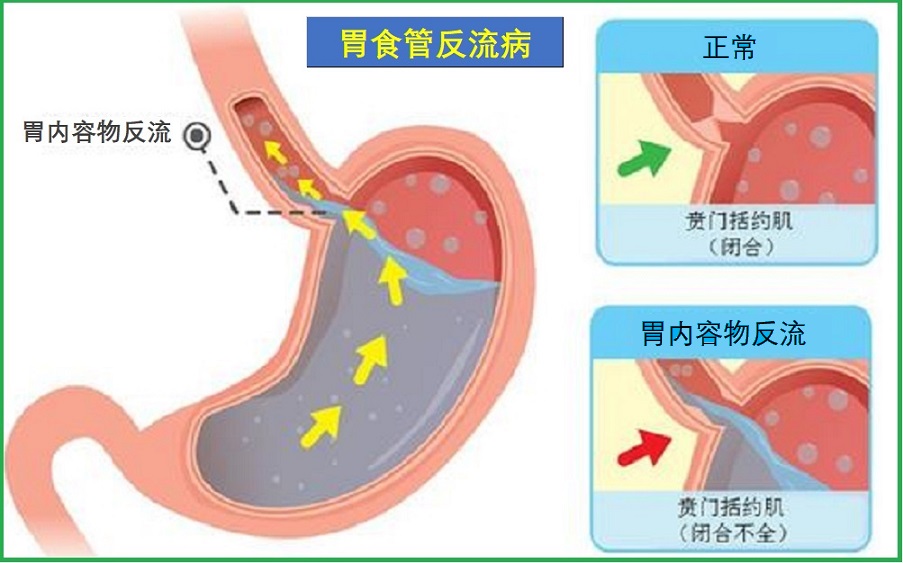
食管下括约肌(LES)是食管和胃之间的一个肌肉环。它可松弛让食物进入胃,然后关闭以防止倒流。但是,某些问题可以使肌肉环不能完全闭合,导致胃酸向上流动,引起胃灼热。导致这些问题可能如下:
- 控制LES的神经失调
- LES肌张力问题
- 蠕动受损
- LES异常的压力
- LES松弛
- 腹部的压力增加
风险因素
可能引起GERD的风险因素包括:- 肥胖
- 吸烟
- 饮酒
- 运动或饭后立即运动
- 饭后躺着、弯腰
- 妊娠
- 之前手术治疗过胃灼热
- 糖尿病
- 硬皮病
- 某些神经系统疾病
- 留置胃管
- 含咖啡因的产品
- 碳酸饮料
- 柑橘类水果
- 巧克力
- 油炸食品
- 辛辣的食物
- 用西红柿做的食品,如比萨饼、或意大利面
- 抗胆碱能药物
- 钙通道阻滞剂
- 茶碱、支气管吸入器,及其他哮喘药物
- 硝酸盐
- 西地那非
- 双膦酸盐
症状
胃灼热和其他消化不良症状,通常发生在暴食后或饱餐一顿后躺下。GERD症状可能持续几分钟或几个小时。
常见症状可能包括如下:
- 烧心感:在开始下胸上移到喉咙处,这是最常见的症状
- 反流:感觉食物返上来
- 在喉咙出现酸、苦的味道
- 打嗝
- 腹胀
- 喉咙痛
- 嘶哑
- 慢性喉炎
- 慢性咳嗽
- 感觉喉咙肿胀
- 醒来感觉窒息
- 吞咽困难
如果有胸痛或其他可能的心脏病发作的症状,立即要求紧急医疗服务,包括如下:
- 胸部挤压或压迫
- 左肩、左臂,或下巴疼痛
- 呼吸困难
- 出汗、皮肤湿冷
- 恶心
- 虚弱
- 头晕
- 开始活动或压力时疼痛
并发症
长期的胃食管反流病可导致并发症,包括如下:- 慢性食管炎和疤痕
- 食管出血和溃疡
- 食管狭窄
- 牙齿问题,这可能是因为胃酸对牙釉质的影响
- 哮喘发作
- 吸入性肺炎:在睡眠中,酸反流到喉咙,可能流入肺部而引起
- 吐血
- 黑色或柏油样大便
- 癌前状态,可导致食管癌的巴雷特食管
- 食管癌
疗法
治疗将取决于胃灼热的原因,重点是防止症状发生和治愈食管的任何损伤。选项可包括如下:
调整饮食和生活方式
- 记住所吃的食物及引起的反应,并给予调整防止烧心症状发生
- 避免引发消化道不适的食物和饮料,如巧克力、辛辣食物、碳酸饮料等
- 饭后至少2-3小时才能运动或躺着
- 减肥、保持健康体重
- 不吸烟
- 避免饮酒,或适度饮酒,限于男性每天饮酒1-2杯,女性1杯
- 避免腰带和衣服太紧,以免腹部承压
- 适当抬高睡眠枕头。
- 限制阿司匹林和非甾体抗炎药使用。
营养与草本综合干预
以下是基于循证医学和循证营养学有关文献综合的结果。
有助于防控胃食管反流病的营养和草本补充剂,主要包括如下:
1.甘草与解甘草素(DGL)提取物:
甘草根是治疗消化道溃疡的一种历史悠久的药物,现代研究继续证实它能够治愈消化道组织。这种非凡能力背后的一些机制现在已经被很好地理解了。甘草植物的化合物增加了侵蚀性病变部位的前列腺素浓度,导致粘液分泌和细胞增殖增加,以帮助愈合。甘草还可以抑制促炎细胞因子如白细胞介素、肿瘤坏死因子和核因子-κB(Nf-κB)的产生;并且是一种强大的氧化应激调节剂。这些特性有助于其保护胃肠道脆弱内壁的能力1-4。
在未精制的甘草根中发现的一种化合物甘草素(Glycyrrhizin),在高剂量下可能会引起副作用,包括腹胀、高血压、低血钾水平、荷尔蒙变化和腹泻。当这些化合物从甘草根中去除时,该成分被称为解甘草素(DGL)提取物。DGL保留了甘草的胃肠道愈合特性,同时避免了大多数副作用5,6。
研究表明,DGL提取物是治疗消化不良的有效药物。在一项随机对照试验中,50名功能性消化不良受试者被随机分配接受安慰剂或75mg已获专利的DGL提取物(Gutgard),每天两次,持续30天。在第15天和第30天,服用GutGard的受试者报告称,与服用安慰剂的人相比,症状总分显著下降。与安慰剂组相比,GutGard组的标准化消化不良评估指数也有显著改善。GutGard是安全的,所有受试者都能很好地耐受7。
2.碳酸盐(钙、镁和钾):
碳酸钙和碳酸镁以及碳酸氢钾可以中和胃酸,多年来一直被用于抗酸剂中8,9。镁和碳酸钙在胃中与盐酸相互作用,形成氯化物盐、水、二氧化碳、氢气和其他良性产物10。
通过中和胃酸,抗酸矿物碳酸盐可以减少对胃肠道脆弱内壁的刺激。抗酸剂还抑制胃酶胃蛋白酶的活性,这种作用还可以防止对溃疡或侵蚀的胃肠道内壁的损伤11。重要的是,对于GERD患者来说,碳酸钙和碳酸镁等抗酸剂可以中和食道中的酸;并且可咀嚼碳酸钙具有相对长的作用持续时间。咀嚼碳酸钙已证明具有改善食道收缩的能力,从而增加酸的清除率12-14。碳酸钙起效迅速,能够在几分钟内缓解GERD症状13。
3.褪黑素:
褪黑素是一种最常与睡眠周期相关的激素,但在肠道中发现的褪黑素水平比在大脑中高出数百倍15。褪黑素有助于减轻自由基和炎症反应造成的损害。褪黑素还有助于保持口腔和食道的粘膜完整性16。褪黑素治疗GERD症状的动物研究发现,它能有效预防酸诱导的食道损伤17。
二项人体试验研究了补充褪黑素对GERD症状的影响。在第一次试验中,176名患者服用了含有6mg褪黑素的多种营养配方。一组175名对照受试者服用PPI(20mg奥美拉唑)。这些影响是通过患者在24小时内无症状(定义为没有烧心或反流)所需的时间来衡量的。褪黑素组的所有患者均报告GERD症状有所改善,而PPI组为三分之二。褪黑素(7天)组的缓解速度比PPI(9天)组更快,副作用发生率更低18。第二项研究将三组9名GERD患者与一组健康对照受试者进行了比较,每组患者采用不同的方案(3mg褪黑素、20mg奥美拉唑或两者兼有)。所有治疗组的胃灼热和胃痛在四周后减轻,8周后完全缓解。然而,只有两个褪黑素组在食管下括约肌功能方面有显著改善19。
4.预防巴雷特食管和食道癌:
GERD增加了导致巴雷特(Barrett)食管的化生(即组织转化)事件的风险,这进一步又显著增加了食道癌的风险。因此,降低这二种严重疾病风险的最有效方法是控制GERD的症状。以下附加的考虑因素也可能是有益的。
几项观察性研究已经检查了饮食模式对Barrett食管或食道癌发病率的影响(独立于GERD)。一些食物和补充剂似乎可以降低癌症和化生的风险。
在一些研究中表明,水果和蔬菜的总摄入量与食管癌风险的降低有关20-22。已经注意到,与柑橘类水果以及黄色、芸苔类或生蔬菜相关的风险降低一直是积极的23,24,20。草莓由于其强大的抗氧化剂,也引起了研究人员对寻找能够保护食道组织的化合物的兴趣。为了验证草莓可能预防食管癌的假设,科学家们给75名食管癌前病变患者服用了冻干草莓粉,为期6个月。冷冻干燥草莓粉每天60g,发现在显微镜检查下改善了食道组织的外观。此外,一些炎症标志物减少,包括环氧合酶-2(COX-2)活性减少63%和Nf-kB活性降低62%。研究人员表示,“我们目前的研究结果表明,冻干草莓粉具有预防人类食管癌症的潜力”25。
来自谷物或全谷物的纤维通常与食管癌症风险降低相关20,26,27。另一方面,动物蛋白、饱和脂肪和膳食胆固醇的消费增加一直导致食管癌症风险增加26,21。
维生素C、维生素E、β-胡萝卜素26,28-30和膳食叶酸26,28,31似乎在大多数研究中降低了食管癌症风险。同样,在一项人群研究中,一般补充剂(即复合维矿素)的使用与风险降低有关32。
一些水果和蔬菜含有一种叫做鞣花酸的强大多酚(抗氧化剂)。它在各种环境中发挥细胞保护作用,并在动物研究中作为食管癌抑制剂以及帮助溃疡愈合得到了充分记录33,34。
锌是许多生物过程中必不可少的微量矿物质,可以预防食道癌35。一项观察性研究评估了60名食管癌或胃癌患者和120名健康对照者的血清锌水平。食管癌患者血清锌水平明显较低。这项研究表明,体内锌水平较低与食管癌的发展相关36。在最近一项关于人类细胞系的实验室研究中,在细胞培养中添加锌可显著抑制食管癌鳞状细胞的增殖。非恶性食管细胞系对锌没有显示出这种显著的抑制反应。此外,锌抑制食管癌细胞增殖的能力在锌螯合剂作用下是可逆的。研究人员发现钙信号的调节是锌介导这种抗癌作用的可能机制37。重要的是,GERD患者经常过度使用质子泵抑制剂,会损害锌的吸收并减少锌在体内的储存38,这突出了这一群体摄入充足锌的重要性。
在癌症的细胞培养或动物模型中研究了各种其他膳食成分,结果呈阳性。其中包括萝卜硫素(来自西兰花)39、含N-乙酰半胱氨酸的维生素E40、原花青素(来自苹果)41和蔓越莓42。在一项研究中,甜菜碱(三甲基甘氨酸)的摄入与Barrett食管的缩小有关28。
更多可查看其个性化的综合干预方案如下:
- 胃食管反流管理(防食管损伤)
- 胃食管反流管理(保护食道)
- 胃食管反流管理(中和胃酸)
- 胃食管反流管理(防药物副作用)
- 胃食管反流管理(防食道癌)
- 胃灼热防控(30-40岁)
- 胃灼热防控(41-50岁)
- 胃灼热防控(51-60岁)
- 胃灼热防控(61岁以上)
以及参阅本网如下专文的相关内容:
医疗干预
常规治疗包括如下:
- 质子泵抑制剂
- H-2受体阻断剂
- 抗酸剂
预防
没有预防胃食道反流病的指南。
参考文献:
1. Baker ME. Licorice and enzymes other than 11 beta-hydroxysteroid dehydrogenase: an evolutionary perspective. Steroids. Feb 1994;59(2):136-141.
2. Furusawa J et al. Glycyrrhiza inflata-derived chalcones, Licochalcone A, Licochalcone B and Licochalcone D, inhibit phosphorylation of NF-kappaB p65 in LPS signaling pathway. International immunopharmacology. Apr 2009;9(4):499-507.
3. Asl MN et al. Review of pharmacological effects of Glycyrrhiza sp. and its bioactive compounds. Phytotherapy research. Jun 2008;22(6):709-724.
4. Aly AM et al. Licorice: a possible anti-inflammatory and anti-ulcer drug. AAPS PharmSciTech. 2005;6(1):E74-82.
5. Larkworthy W et al. Deglycyrrhizinized liquorice in the treatment of chronic duodenal ulcer. A retrospective endoscopic survey of 32 patients. The Practitioner. Dec 1975;215(1290):787-792.
6. Isbrucker RA et al. Risk and safety assessment on the consumption of Licorice root (Glycyrrhiza sp.), its extract and powder as a food ingredient, with emphasis on the pharmacology and toxicology of glycyrrhizin. Regulatory toxicology and pharmacology. Dec 2006;46(3):167-192.
7. Raveendra KR et al. An Extract of Glycyrrhiza glabra (GutGard) Alleviates Symptoms of Functional Dyspepsia: A Randomized, Double-Blind, Placebo-Controlled Study. Evidence-based complementary and alternative medicine. 2012;2012:216970.
8. Maton PN et al. Antacids revisited: a review of their clinical pharmacology and recommended therapeutic use. Drugs. Jun 1999;57(6):855-870.
9. Gold Standard. Drug Monograph. Citric Acid; Potassium Bicarbonate; Sodium Bicarbonate. www.clinicalkey.com. Last updated 6/30/2002. Accessed 2/22/2016.
10. The American Society of Health-System Pharmacists I. Aluminum Hydroxide and Magnesium Hydroxide. https://www.nlm.nih.gov/medlineplus/druginfo/meds/a601013.html. Accessed 2/15/2016.
11. Gold Standard. Drug Monograph. Calcium Carbonate. www.clinicalkey.com. Last updated 12/30/2009. Accessed 2/22/2016.
12. McRorie JW et al. Evidence-based treatment of frequent heartburn: the benefits and limitations of over-the-counter medications. Journal of the American Association of Nurse Practitioners. Jun 2014;26(6):330-339.
13. Robinson M et al. Effects of antacid formulation on postprandial oesophageal acidity in patients with a history of episodic heartburn. Alimentary pharmacology & therapeutics. Mar 2002;16(3):435-443.
14. Rodriguez-Stanley S et al. Calcium carbonate antacids alter esophageal motility in heartburn sufferers. Digestive diseases and sciences. Nov-Dec 2004;49(11-12):1862-1867.
15. Werbach MR. Melatonin for the treatment of gastroesophageal reflux disease. Altern Ther Health Med. 2008;14(4):54–58.
16. Brzozowska I et al. Mechanisms of esophageal protection, gastroprotection and ulcer healing by melatonin. implications for the therapeutic use of melatonin in gastroesophageal reflux disease (GERD) and peptic ulcer disease. Curr Pharm Des. 2014;20(30):4807-15.
17. Konturek SJ et al. Protective influence of melatonin against acute esophageal lesions involves prostaglandins, nitric oxide and sensory nerves. J. Physiol. Pharmacol. 2007;58(2):361–377.
18. Pereira Rde S. Regression of gastroesophageal reflux disease symptoms using dietary supplementation with melatonin, vitamins and aminoacids: comparison with omeprazole. J. Pineal Res. 2006;41(3):195–200.
19. Kandil TS et al. The potential therapeutic effect of melatonin in Gastro-Esophageal Reflux Disease. BMC Gastroenterol. 2010;10:7.
20. Chen H et al. Dietary patterns and adenocarcinoma of the esophagus and distal stomach. Am J Clin Nutr. 2002;75(1):137–144.
21. Navarro Silvera SA et al. Food group intake and risk of subtypes of esophageal and gastric cancer. Int J Cancer. 2008;123(4):852–860.
22. Navarro Silvera SA et al. Principal component analysis of dietary and lifestyle patterns in relation to risk of subtypes of esophageal and gastric cancer. Ann Epidemiol. 2011;21(7):543–550.
23. Gonzalez CA et al. Fruit and vegetable intake and the risk of stomach and oesophagus adenocarcinoma in the European Prospective Investigation into Cancer and Nutrition (EPIC-EURGAST). Int J Cancer. 2006;118(10):2559–2566.
24. Steevens J et al. Vegetables and fruits consumption and risk of esophageal and gastric cancer subtypes in the Netherlands Cohort Study. Int J Cancer. 2011;129(11):2681–2693.
25. Chen T et al. Randomized phase II trial of lyophilized strawberries in patients with dysplastic precancerous lesions of the esophagus. Cancer Prev Res (Phila). 2012 Jan;5(1):41-50.
26. Mayne ST et al. Nutrient intake and risk of subtypes of esophageal and gastric cancer. Cancer Epidemiol Biomarkers Prev. 2001;10(10):1055–1062.
27. Terry P et al. Inverse association between intake of cereal fiber and risk of gastric cardia cancer. Gastroenterology. 2001;120(2):387-91.
28. Bollschweiler E et al. Vitamin intake and risk of subtypes of esophageal cancer in Germany. J. Cancer Res. Clin. Oncol. 2002;128(10):575–580.
29. Kubo A et al. Meta-analysis of antioxidant intake and the risk of esophageal and gastric cardia adenocarcinoma. Am J Gastroenterol. 2007;102(10):2323–30; quiz 2331.
30. Carman S et al. Vitamin E intake and risk of esophageal and gastric cancers in the NIH-AARP Diet and Health Study. Int J Cancer. 2009;125(1):165–170.
31. Ibiebele TI et al. High intake of folate from food sources is associated with reduced risk of esophageal cancer in an Australian population. Journal of Nutrition. 2011;141(2):274–283.
32. Dong LM et al. Dietary supplement use and risk of neoplastic progression in esophageal adenocarcinoma: a prospective study. Nutr Cancer. 2008;60(1):39–48.
33. Whitley AC et al. The dietary polyphenol ellagic acid is a potent inhibitor of hOAT1. Drug Metab Dispos. 2005 Aug;33(8):1097-100.
34. Beserra AM, Calegari PI, Souza Mdo C, et al. Gastroprotective and ulcer-healing mechanisms of ellagic acid in experimental rats. J Agric Food Chem. 2011 Jul 13;59(13):6957-65.
35. Grosvenor S. Nutrition: Science and Applications. Vol 1: Saunders College Publishing; 1995.
36. Hashemi SM et al. The Relationship between Serum Selenium and Zinc with Gastroesophageal Cancers in the Southeast of Iran. Indian journal of medical and paediatric oncology. Apr-Jun 2017;38(2):169-172.
37. Choi S et al. Selective inhibitory effects of zinc on cell proliferation in esophageal squamous cell carcinoma through Orai1. FASEB journal. 2018 Jan;32(1):404-416.
38. Farrell CP et al. Proton Pump Inhibitors Interfere With Zinc Absorption and Zinc Body Stores. Gastroenterology research.Dec 2011;4(6):243-251.
39. Qazi A et al. Anticancer activity of a broccoli derivative, sulforaphane, in barrett adenocarcinoma: potential use in chemoprevention and as adjuvant in chemotherapy. Transl Oncol. 2010;3(6):389–399.
40. Hao J et al. Effect of alpha-tocopherol, N-acetylcysteine and omeprazole on esophageal adenocarcinoma formation in a rat surgical model. Int J Cancer. 2009;124(6):1270–1275.
41. Pierini R et al. Procyanidin effects on oesophageal adenocarcinoma cells strongly depend on flavan-3-ol degree of polymerization. Mol. Nutr. Food Res. 2008;52(12):1399–1407.
42. Kresty LA et al. Cranberry proanthocyanidins induce apoptosis and inhibit acid-induced proliferation of human esophageal adenocarcinoma cells. J Agric Food Chem. 2008;56(3):676–680.
参考来源:
美国梅奥诊所
www.mayoclinic.org
美国胃肠病协会
http://www.gastro.org
美国国立糖尿病、消化及肾病研究所
http://www.niddk.nih.gov
加拿大健康信息研究所
http://www.cihi.ca
加拿大卫生部
http://www.hc-sc.gc.ca
免责声明和安全信息
- 本信息(包括任何附带资料)不是为了取代医生或有关合格从业人士的建议或忠告。
- 任何人如果想要对本文涉及的药物、饮食、运动或其他生活方式的使用、或改变调整,以预防或治疗某一特定健康状况或疾病,应首先咨询医生或有关合格从业人士,并获得他/她们的许可。妊娠和哺乳妇女在使用本网站任何内容前,尤其应征求医生的意见。
- 除非另有说明,本网站所述内容仅适用于成人。
- 本网站所推荐的任何产品,消费者应该以实际的产品标签内容为准,尤其应关注重要的安全信息以及产品最新信息,包括剂量、使用方法和禁忌症等。
- 由于循证医学研究、文献及有关产品处于不断的变化中,本网站工作人员将尽力更新。
- 本网站不能保证所载文章内容、综合干预方案以及相关成分或产品述及的健康益处,也不承担任何责任。